W gabinecie lekarza rodzinnego Terapia 2018, 9 ( 368 ) : 15 - 24
Zapalenia zatok – codzienny problem w gabinecie lekarza rodzinnego
Sinusitis – a common problem in family doctor’s practice
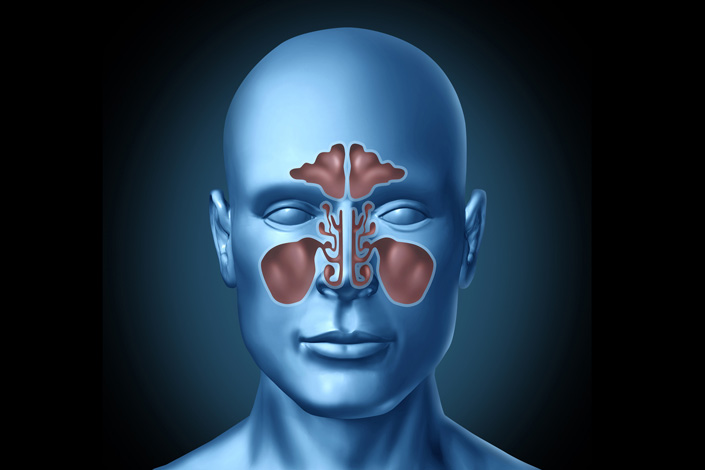
Zapalenia zatok przynosowych należą do najczęściej występujących chorób w populacji. Stanowią przyczynę istotnego odsetka wizyt, zarówno w gabinetach lekarzy rodzinnych, jak i lekarzy specjalistów. Mając na uwadze wzajemne związki anatomiczne i czynnościowe zatok przynosowych i nosa, praktycznie każdemu zapaleniu błony śluzowej zatok przynosowych (sinusitis), towarzyszy zapalenie błony śluzowej nosa (rhinitis), gdyż pod względem fizjologicznym i patofizjologicznym oba te obszary stanowią integralną całość. Dlatego też, od kilkunastu lat w literaturze dla tego schorzenia przyjęto nazwę rhinosinusitis, czyli zapalenie błony śluzowej nosa i zatok przynosowych (rycina 1). Wyjątek stanowią zapalenia zębopochodne, czy odczyn zapalny związany z guzem zatok przynosowych, gdzie zapalenie może być ograniczone wyłącznie do wnętrza danej zatoki i nie musi tym procesom towarzyszyć stan zapalny błony śluzowej nosa (1,2).
Zaloguj się i przeczytaj bezpłatnie całą treść artykułu.
Nie masz jeszcze konta dostępowego?
Zarejestruj się bezpłatnie, a otrzymasz:
* dostęp do wszystkich doniesień oraz pełnych tekstów artykułów naukowych w naszej Czytelni,
* prawo do bezpłatnego otrzymywania newslettera "Aktualności TERAPIA" z przeglądem interesujących i przydatnych wiadomości ze świata medycyny oraz systemu ochrony zdrowia w Polsce i na świecie,
* możliwość komentowania bieżących wydarzeń oraz udziału w ciekawych quizach i konkursach.
Zapraszamy serdecznie, dołącz do naszej społeczności.
Dodaj komentarz